


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Mechanism of action: Bortezomib is a proteasome inhibitor. It is specifically designed to inhibit the chymotrypsin-like activity of the 26S proteasome in mammalian cells. The 26S proteasome is a large protein complex that degrades ubiquitinated proteins. The ubiquitin-proteasome pathway plays an essential role in regulating the turnover of specific proteins, thereby maintaining homeostasis within cells. Inhibition of the 26S proteasome prevents this targeted proteolysis and affects multiple signalling cascades within the cell, ultimately resulting in cancer cell death.
Bortezomib is highly selective for the proteasome. At 10 μM concentrations, Bortezomib does not inhibit any of a wide variety of receptors and proteases screened and is more than 1,500-fold more selective for the proteasome than for its next preferable enzyme. The kinetics of proteasome inhibition were evaluated in vitro, and Bortezomib was shown to dissociate from the proteasome with a t½of 20 minutes, thus demonstrating that proteasome inhibition by Bortezomib is reversible.
Bortezomib mediated proteasome inhibition affects cancer cells in a number of ways, including, but not limited to, altering regulatory proteins, which control cell cycle progression and nuclear factor kappa B (NF-kB) activation. Inhibition of the proteasome results in cell cycle arrest and apoptosis. NF-kB is a transcription factor whose activation is required for many aspects of tumourigenesis, including cell growth and survival, angiogenesis, cell-cell interactions, and metastasis. In myeloma, Bortezomib affects the ability of myeloma cells to interact with the bone marrow microenvironment.
Experiments have demonstrated that Bortezomib is cytotoxic to a variety of cancer cell types and that cancer cells are more sensitive to the pro-apoptotic effects of proteasome inhibition than normal cells. Bortezomib causes reduction of tumour growth in vivo in many preclinical tumour models, including multiple myeloma.
Data from in vitro, ex-vivo, and animal models with Bortezomib suggest that it increases osteoblast differentiation and activity and inhibits osteoclast function. These effects have been observed in patients with multiple myeloma affected by an advanced osteolytic disease and treated with Bortezomib.
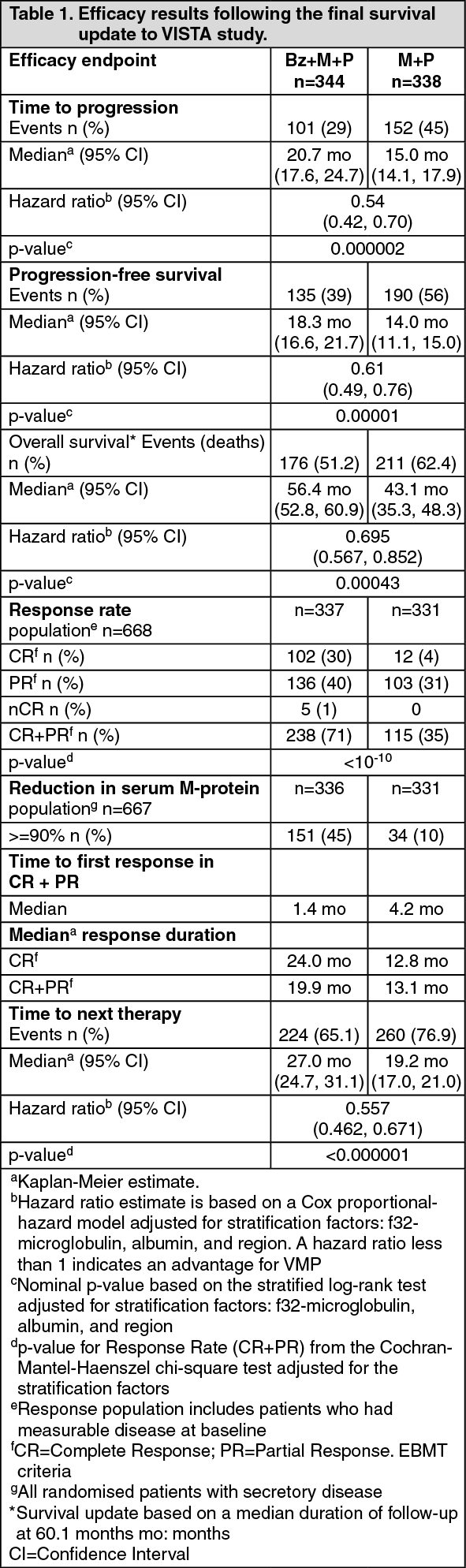
Clinical efficacy in previously untreated multiple myeloma: A prospective Phase III, international, randomised (1:1), open-label clinical study (MMY-3002 VISTA) of 682 patients was conducted to determine whether Bortezomib (1.3 mg/m2 injected intravenously) in combination with melphalan (9 mg/m2) and prednisone (60 mg/m2) resulted in improvement in time to progression (TTP) when compared to melphalan (9 mg/m2) and prednisone (60 mg/m2) in patients with previously untreated multiple myeloma. Treatment was administered for a maximum of 9 cycles (approximately 54 weeks) and was discontinued early for disease progression or unacceptable toxicity. The median age of the patients in the study was 71 years, 50% were male, 88% were Caucasian and the median Karnofsky performance status score for the patients was 80. Patients had IgG/IgA/Light chain myeloma in 63%/25%/8% instances, a median hemoglobin of 105 g/L, and a median platelet count of 221.5 x 109/L. Similar proportions of patients had creatinine clearance ≤ 30 mL/min (3% in each arm).
At the time of a pre-specified interim analysis, the primary endpoint, time to progression, was met and patients in the M+P arm were offered Bz+M+P treatment. Median follow-up was 16.3 months. The final survival update was performed with a median duration of follow-up of 60.1 months. A statistically significant survival benefit in favour of the Bz+M+P treatment group was observed (HR=0.695; p=0.00043) despite subsequent therapies including Bortezomib-based regimens. Median survival for the Bz+M+P treatment group was 56.4 months compared to 43.1 for the M+P treatment group. Efficacy results are presented in Table 1: See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePatients eligible for stem cell transplantation: Two randomised, open-label, multicenter Phase III trials (IFM-2005-01, MMY-3010) were conducted to demonstrate the safety and efficacy of Bortezomib in dual and triple combinations with other chemotherapeutic agents, as induction therapy prior to stem cell transplantation in patients with previously untreated multiple myeloma.
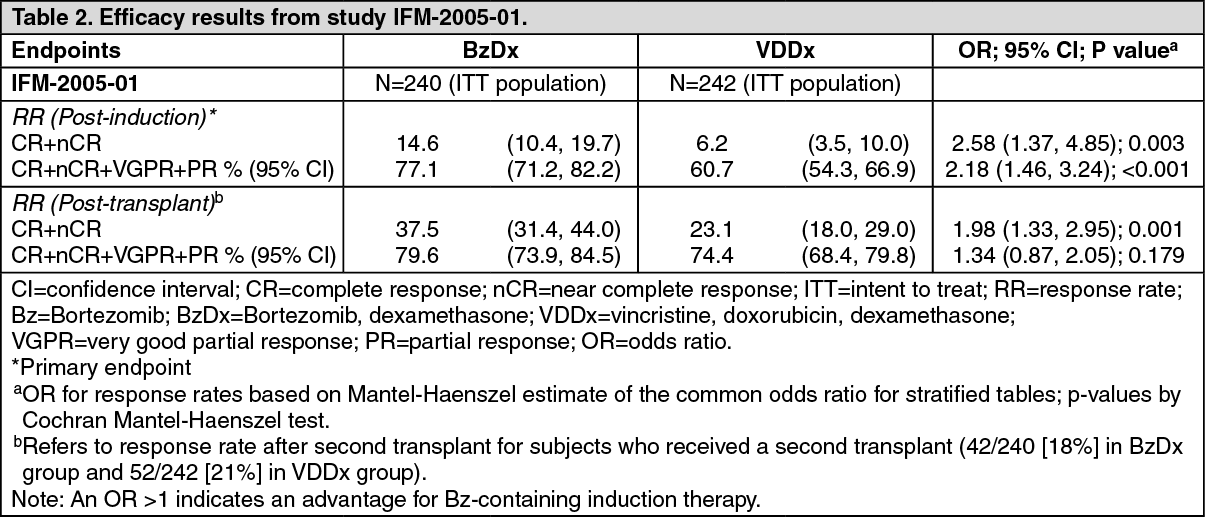
In study IFM-2005-01 Bortezomib combined with dexamethasone [BzDx, n=240] was compared to vincristine-doxorubicin-dexamethasone [VDDx, n=242]. Patients in the BzDx group received four 21-day cycles, each consisting of Bortezomib (1.3 mg/m2 administered intravenously twice weekly on days 1, 4, 8, and 11), and oral dexamethasone (40 mg/day on days 1 to 4 and days 9 to 12, in Cycles 1 and 2, and on days 1 to 4 in Cycles 3 and 4).
Autologous stem cell transplants were received by 198 (82%) patients and 208 (87%) patients in the VDDx and BzDx groups respectively; the majority of patients underwent one single transplant procedure. Patient demographic and baseline disease characteristics were similar between the treatment groups. Median age of the patients in the study was 57 years, 55% were male and 48% of patients had high-risk cytogenetics. The median duration of treatment was 13 weeks for the VDDx group and 11 weeks for the BzDx group. The median number of cycles received for both groups was 4 cycles.
The primary efficacy endpoint of the study was post-induction response rate (CR+nCR). A statistically significant difference in CR+nCR was observed in favour of the Bortezomib combined with dexamethasone group. Secondary efficacy endpoints included post-transplant response rates (CR+nCR, CR+nCR+VGPR+PR), Progression Free Survival and Overall Survival. Main efficacy results are presented in Table 2. (See Table 2.)
 Click on icon to see table/diagram/image
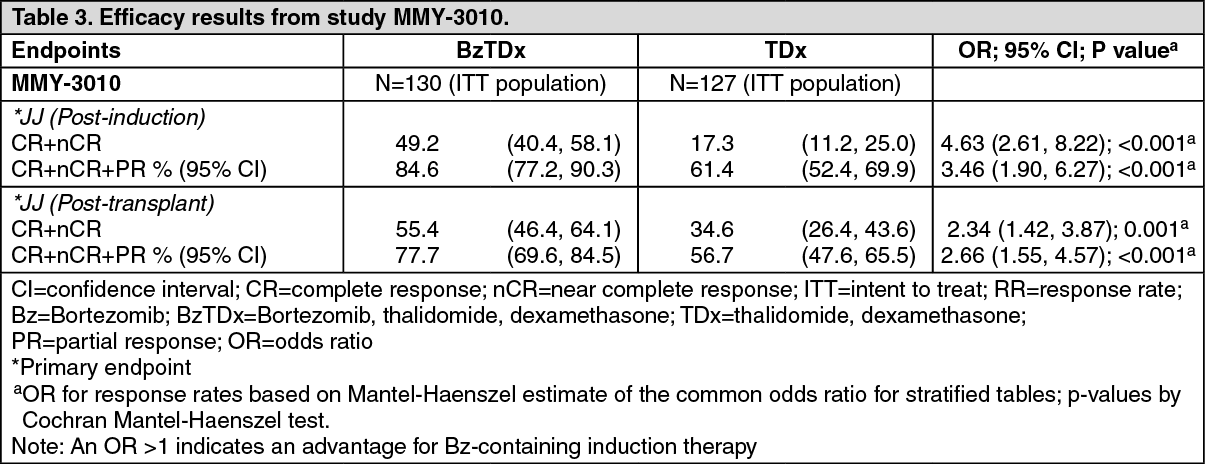
Click on icon to see table/diagram/imageIn study MMY-3010 induction treatment with Bortezomib combined with thalidomide and dexamethasone [BzTDx, n=130] was compared to thalidomide-dexamethasone [TDx, n=127]. Patients in the BzTDx group received six 4-week cycles, each consisting of Bortezomib (1.3 mg/m2 administered twice weekly days 1, 4, 8, and 11, followed by a 17-day rest period from day 12 to day 28), dexamethasone (40 mg administered orally on days 1 to 4 and days 8 to 11), and thalidomide (administered orally at 50 mg daily on days 1-14, increased to 100 mg on days 15-28 and thereafter to 200 mg daily).
One single autologous stem cell transplant was received by 105 (81%) patients and 78 (61%) patients in the BzTDx and TDx groups, respectively. Patient demographic and baseline disease characteristics were similar between the treatment groups. Patients in the BzTDx and TDx groups respectively had a median age of 57 versus 56 years, 99% versus 98% patients were Caucasians, and 58% versus 54% were males. In the BzTDx group 12% of patients were cytogenetically classified as high risk versus 16% of patients in the TDx group. The median duration of treatment was 24.0 weeks and the median number of treatment cycles received was 6.0, and was consistent across treatment groups.
The primary efficacy endpoints of the study were post-induction and post-transplant response rates (CR+nCR). A statistically significant difference in CR+nCR was observed in favour of the Bortezomib combined with dexamethasone and thalidomide group. Secondary efficacy endpoints included Progression Free Survival and Overall Survival. Main efficacy results are presented in Table 3. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageClinical efficacy in relapsed or refractory multiple myeloma: The safety and efficacy of Bortezomib (injected intravenously) were evaluated in 2 studies at the recommended dose of 1.3 mg/m2: a Phase III randomised, comparative study (APEX), versus dexamethasone (Dex), of 669 patients with relapsed or refractory multiple myeloma who had received 1-3 prior lines of therapy, and a Phase II single-arm study of 202 patients with relapsed and refractory multiple myeloma, who had received at least 2 prior lines of treatment and who were progressing on their most recent treatment.
In the Phase III study, treatment with Bortezomib led to a significantly longer time to progression, a significantly prolonged survival and a significantly higher response rate, compared to treatment with dexamethasone (see Table 4), in all patients as well as in patients who have received 1 prior line of therapy. As a result of a pre-planned interim analysis, the dexamethasone arm was halted at the recommendation of the data monitoring committee and all patients randomised to dexamethasone were then offered Bortezomib, regardless of disease status. Due to this early crossover, the median duration of follow-up for surviving patients is 8.3 months. Both in patients who were refractory to their last prior therapy and those who were not refractory, overall survival was significantly longer and response rate was significantly higher on the Bortezomib arm.
Of the 669 patients enrolled, 245 (37%) were 65 years of age or older. Response parameters as well as TTP remained significantly better for Bortezomib independently of age. Regardless of β2-microglobulin levels at baseline, all efficacy parameters (time to progression and overall survival, as well as response rate) were significantly improved on the Bortezomib arm.
In the refractory population of the Phase II study, responses were determined by an independent review committee and the response criteria were those of the European Bone Marrow Transplant Group. The median survival of all patients enrolled was 17 months (range <1 to 36+ months). This survival was greater than the six-to-nine month median survival anticipated by consultant clinical investigators for a similar patient population. By multivariate analysis, the response rate was independent of myeloma type, performance status, chromosome 13 deletion status, or the number or type of previous therapies. Patients who had received 2 to 3 prior therapeutic regimens had a response rate of 32% (10/32) and patients who received greater than 7 prior therapeutic regimens had a response rate of 31% (21/67). (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the Phase II study, patients who did not obtain an optimal response to therapy with Bortezomib alone were able to receive high-dose dexamethasone in conjunction with Bortezomib. The protocol allowed patients to receive dexamethasone if they had had a less than optimal response to Bortezomib alone. A total of 74 evaluable patients were administered dexamethasone in combination with Bortezomib. Eighteen percent of patients achieved, or had an improved response [MR (11%) or PR (7%)] with combination treatment.
Clinical efficacy with subcutaneous administration of Bortezomib in patients with relapsed/refractory multiple myeloma: An open label, randomised, Phase III non-inferiority study compared the efficacy and safety of the subcutaneous administration of Bortezomib versus the intravenous administration. This study included 222 patients with relapsed/refractory multiple myeloma, who were randomised in a 2:1 ratio to receive 1.3 mg/m2 of Bortezomib by either the subcutaneous or intravenous route for 8 cycles. Patients who did not obtain an optimal response (less than Complete Response [CR]) to therapy with Bortezomib alone after 4 cycles were allowed to receive dexamethasone 20 mg daily on the day of and after Bortezomib administration. Patients with baseline Grade ≥ 2 peripheral neuropathy or platelet counts <50,000/μl were excluded. A total of 218 patients were evaluable for response.
This study met its primary objective of non-inferiority for response rate (CR+PR) after 4 cycles of single agent Bortezomib for both the subcutaneous and intravenous routes, 42% in both groups. In addition, secondary response-related and time to event related efficacy endpoints showed consistent results for subcutaneous and intravenous administration (Table 5). (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageBortezomib combination treatment with pegylated liposomal doxorubicin (study DOXIL-MMY-3001): A Phase III randomised, parallel-group, open-label, multicentre study was conducted in 646 patients comparing the safety and efficacy of Bortezomib plus pegylated liposomal doxorubicin versus Bortezomib monotherapy in patients with multiple myeloma who had received at least 1 prior therapy and who did not progress while receiving anthracycline-based therapy. The primary efficacy endpoint was TTP while the secondary efficacy endpoints were OS and ORR (CR+PR), using the European Group for Blood and Marrow Transplantation (EBMT) criteria.
A protocol-defined interim analysis (based on 249 TTP events) triggered early study termination for efficacy. This interim analysis showed a TTP risk reduction of 45% (95% CI; 29-57 %, p <0.0001) for patients treated with combination therapy of Bortezomib and pegylated liposomal doxorubicin. The median TTP was 6.5 months for the Bortezomib monotherapy patients compared with 9.3 months for the Bortezomib plus pegylated liposomal doxorubicin combination therapy patients. These results, though not mature, constituted the protocol defined final analysis.
Bortezomib combination treatment with dexamethasone: In the absence of any direct comparison between Bortezomib and Bortezomib in combination with dexamethasone in patients with progressive multiple myeloma, a statistical matched-pair analysis was conducted to compare results from the non randomised arm of Bortezomib in combination with dexamethasone (Phase II open-label study MMY-2045), with results obtained in the Bortezomib monotherapy arms from different Phase III randomised studies (M34101-039 [APEX] and DOXIL MMY-3001) in the same indication.
The matched-pair analysis is a statistical method in which patients in the treatment group (e.g. Bortezomib in combination with dexamethasone) and patients in the comparison group (e.g. Bortezomib) are made comparable with respect to confounding factors by individually pairing study subjects. This minimises the effects of observed confounders when estimating treatment effects using non-randomised data.
One hundred and twenty seven matched pairs of patients were identified. The analysis demonstrated improved ORR (CR+PR) (odds ratio 3.769; 95% CI 2.045-6.947; p <0.001), PFS (hazard ratio 0.511; 95% CI 0.309-0.845; p=0.008), TTP (hazard ratio 0.385; 95% CI 0.212-0.698; p=0.001) for bortezomib in combination with dexamethasone over Bortezomib mono-therapy.
Limited information on Bortezomib retreatment in relapsed multiple myeloma is available.
Phase II study MMY-2036 (RETRIEVE), single arm, open-label study was conducted to determine the efficacy and safety of retreatment with Bortezomib. One hundred and thirty patients (≥18 years of age) with multiple myeloma who previously had at least partial response on a Bortezomib-containing regimen were retreated upon progression. At least 6 months after prior therapy, Bortezomib was started at the last tolerated dose of 1.3 mg/m2 (n=93) or ≤1.0 mg/m2 (n=37) and given on days 1, 4, 8 and 11 every 3 weeks for maximum of 8 cycles either as single agent or in combination with dexamethasone in accordance with the standard of care. Dexamethasone was administered in combination with Bortezomib to 83 patients in Cycle 1 with an additional 11 patients receiving dexamethasone during the course of Bortezomib retreatment cycles.
The primary endpoint was best confirmed response to retreatment as assessed by EBMT criteria. The overall best response rate (CR + PR), to retreatment in 130 patients was 38.5% (95% CI: 30.1, 47.4).
Patients with previously treated light-chain (AL) Amyloidosis: An open label non randomised Phase I/II study was conducted to determine the safety and efficacy of Bortezomib in patients with previously treated light-chain (AL) Amyloidosis. No new safety concerns were observed during the study, and in particular Bortezomib did not exacerbate target organ damage (heart, kidney and liver). In an exploratory efficacy analysis, a 67.3% response rate (including a 28.6% CR rate) as measured by hematologic response (M-protein) was reported in 49 evaluable patients treated with the maximum allowed doses of 1.6 mg/m2 weekly and 1.3 mg/m2 twice-weekly. For these dose cohorts, the combined 1-year survival rate was 88.1%.
Paediatric population: The European Medicines Agency has waived the obligation to submit the results of studies with Bortezomib in all subsets of the paediatric population in multiple myeloma.
Pharmacokinetics: Absorption: Following intravenous bolus administration of a 1.0 mg/m2 and 1.3 mg/m2 dose to 11 patients with multiple myeloma and creatinine clearance values greater than 50 mL/min, the mean first-dose maximum plasma concentrations of Bortezomib were 57 and 112 ng/mL, respectively. In subsequent doses, mean maximum observed plasma concentrations ranged from 67 to 106 ng/mL for the 1.0 mg/m2 dose and 89 to 120 ng/mL for the 1.3 mg/m2 dose.
Following an intravenous bolus or subcutaneous injection of a 1.3 mg/m2 dose to patients with multiple myeloma (n=14 in the intravenous group, n=17 in the subcutaneous group), the total systemic exposure after repeat dose administration (AUClast) was equivalent for subcutaneous and intravenous administrations. The Cmax after subcutaneous administration (20.4 ng/mL) was lower than intravenous (223 ng/mL). The AUClast geometric mean ratio was 0.99 and 90% confidence intervals were 80.18%-122.80%.
Distribution: The mean distribution volume (Vd) of Bortezomib ranged from 1,659 L to 3,294 L following single- or repeated-dose intravenous administration of 1.0 mg/m2 or 1.3 mg/m2 to patients with multiple myeloma. This suggests that Bortezomib distributes widely to peripheral tissues. Over a Bortezomib concentration range of 0.01 to 1.0 μg/mL, the in vitro protein binding averaged 82.9% in human plasma. The fraction of Bortezomib bound to plasma proteins was not concentration-dependent.
Biotransformation: In vitro studies with human liver microsomes and human cDNA-expressed cytochrome P450 isozymes indicate that bortezomib is primarily oxidatively metabolised via cytochrome P450 enzymes, 3A4, 2C19, and 1A2. The major metabolic pathway is deboronation to form two deboronated metabolites that subsequently undergo hydroxylation to several metabolites. Deboronated-bortezomib metabolites are inactive as 26S proteasome inhibitors.
Elimination: The mean elimination half-life (t½) of Bortezomib upon multiple dosing ranged from 40-193 hours. Bortezomib is eliminated more rapidly following the first dose compared to subsequent doses. Mean total body clearances were 102 and 112 L/h following the first dose for doses of 1.0 mg/m2 and 1.3 mg/m2, respectively, and ranged from 15 to 32 L/h and 18 to 32 L/h following subsequent doses for doses of 1.0 mg/m2 and 1.3 mg/m2, respectively.
Special populations: Hepatic impairment: The effect of hepatic impairment on the pharmacokinetics of Bortezomib was assessed in a Phase I study during the first treatment cycle, including 61 patients primarily with solid tumors and varying degrees of hepatic impairment at Bortezomib doses ranging from 0.5 to 1.3 mg/m2.
When compared to patients with normal hepatic function, mild hepatic impairment did not alter dose-normalised Bortezomib AUC. However, the dose-normalised mean AUC values were increased by approximately 60% in patients with moderate or severe hepatic impairment. A lower starting dose is recommended in patients with moderate or severe hepatic impairment, and those patients should be closely monitored (see Table 10 under Dosage & Administration).
Renal impairment: A pharmacokinetic study was conducted in patients with various degrees of renal impairment who were classified according to their creatinine clearance values (CrCL) into the following groups: Normal (CrCL ≥ 60 mL/min/1.73 m2, n=12), Mild (CrCL=40-59 mL/min/1.73 m2, n=10), Moderate (CrCL=20-39 mL/min/1.73 m2, n=9), and Severe (CrCL < 20 mL/min/1.73 m2, n=3). A group of dialysis patients who were dosed after dialysis was also included in the study (n=8). Patients were administered intravenous doses of 0.7 to 1.3 mg/m2 of Bortezomib twice weekly. Exposure of Bortezomib (dose-normalised AUC and Cmax) was comparable among all the groups.
Toxicology: Preclinical safety data: Bortezomib was positive for clastogenic activity (structural chromosomal aberrations) in the in vitro chromosomal aberration assay using Chinese hamster ovary (CHO) cells at concentrations as low as 3.125 μg/mL, which was the lowest concentration evaluated. Bortezomib was not genotoxic when tested in the in vitro mutagenicity assay (Ames assay) and in vivo micronucleus assay in mice.
Developmental toxicity studies in the rat and rabbit have shown embryo-fetal lethality at maternally toxic doses, but no direct embryo-foetal toxicity below maternally toxic doses. Fertility studies were not performed but evaluation of reproductive tissues has been performed in the general toxicity studies. In the 6-month rat study, degenerative effects in both the testes and the ovary have been observed. It is, therefore, likely that Bortezomib could have a potential effect on either male or female fertility. Peri- and postnatal development studies were not conducted.
In multi-cycle general toxicity studies conducted in the rat and monkey, the principal target organs included the gastrointestinal tract, resulting in vomiting and/or diarrhoea; haematopoietic and lymphatic tissues, resulting in peripheral blood cytopenias, lymphoid tissue atrophy and haematopoietic bone marrow hypocellularity; peripheral neuropathy (observed in monkeys, mice and dogs) involving sensory nerve axons; and mild changes in the kidneys. All these target organs have shown partial to full recovery following discontinuation of treatment.
Based on animal studies, the penetration of Bortezomib through the blood-brain barrier appears to be limited, if any and the relevance to humans is unknown.
Cardiovascular safety pharmacology studies in monkeys and dogs show that intravenous doses approximately two to three times the recommended clinical dose on a mg/m2 basis are associated with increases in heart rate, decreases in contractility, hypotension and death. In dogs, the decreased cardiac contractility and hypotension responded to acute intervention with positive inotropic or pressor agents. Moreover, in dog studies, a slight increase in the corrected QT interval was observed.